Sick Building Syndrome and Building Related Illness

Sick Building Syndrome and Building Related Illness
What is the Difference?

Do Buildings Get Sick?
Sick Building Syndrome and Building Related Illness are two distinct diagnoses. People often use the term “sick building” when referring to a property, but buildings don’t get sick – people do. I believe if there are numerous people suffering from Sick Building Syndrome (SBS) it’s okay to refer to the building as “sick,” but that’s technically inaccurate. So what is the difference between SBS and Building Related Illness (BRI)?
Sick Building Syndrome (SBS)
Sick Building Syndrome includes the following symptomology:
- complaints of acute discomfort (.e.g, headache; eye, nose or throat irritation, dry cough, dry or itchy skin, dizziness and nausea, difficulty concentrating,fatigue, sensitivity to odors, and rash)
- unknown cause of symptoms
- most symptoms vanish shortly after occupants leave the building
A rule of thumb states unless 20% or more of occupants are suffering Sick Building Syndrome symptoms, it is not SBS. I think this is a terrible rule of thumb, and it really only benefits occupants in smaller buildings. If you were suffering these symptoms in a household of 3 it’s automatically Sick Building Syndrome. But if you and 198 other occupants are suffering an office building of 1,000 – it’s automatically not SBS? That’s ridiculous. If 199 people are suffering in any building you better start to believe there’s a serious problem. The 20% rule just doesn’t add up.
Building Related Illness (BRI)
Building Related Illness is, by definition, different than Sick Building Syndrome. Building Related Illness is generally allergic reactions or infections. Symptoms and patterns are as follows:
- complaints of specific symptoms such as cough, chest tightness, fever, chills, and muscle aches
- symptoms can be clinically defined
- cause of symptoms is known
- complaints can continue after having left the building

Building Related Illness is different than Sick Building Syndrome
This sort of case might sound familiar. Think post-Katrina FEMA cottages, Chinese drywall or Chinese flooring with formaldehyde.
Humidifier fever, Legionnaires Disease, skin rashes, hypersensitivity pneumonitis, and other illness related to bacteria, fungus (mold), and viruses are often classified as Building Related Illnesses, not Sick Building Syndrome.
Often the words “malaise” and “lethargy” are used during BRI or SBS interviews. According to Managing Indoor Air Quality, “malaise is a vague feeling of uneasiness or physical discomfort,” and “lethargy is characterized by abnormal drowsiness or torpor, apathy, sluggishness and great lack of energy.”
At the heart of every Sick Building Syndrome Inspection is an occupant survey that helps investigators understand symptoms and develop hypotheses about what in the building could be causing these symptoms.
Indoor Air Quality and Sick Building Syndrome
Indoor air quality is almost always associated with Sick Building Syndrome (and Building Related Illness). Whether from insufficient ventilation, excessive accumulation of indoor air pollutants, or a combination thereof, IAQ is almost always intimately tied to the symptoms of Sick Building Syndrome or Building Related Illness.
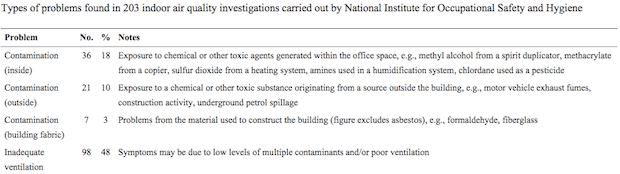
Excerpt Chart from NIOSH – Types of Problems with Sick Building Syndrome
Ventilation is a crucial element in maintaining good IAQ. Point source exhaust for known sources of contaminants (e.g., combustion appliances, paint/chemistry hoods, etc.) and moisture (e.g., stove top, shower, indoor pool, etc.) is a relatively easy way to reduce indoor pollutants. But when these systems are broken or occupants don’t know to operate them rapid accumulation of indoor pollutants can lead to Sick Building Syndrome.
The other half of the ventilation equation is the introduction of outside air. As we continue building better sealed buildings for energy efficiency, we must ensure sufficient outside air delivery. If you have a carbon dioxide (CO2) meter and watch it as an unventilated room fills with occupants you can see CO2 levels rise quickly. CO2 can be used as an indicator for measuring ventilation effectiveness.
Indoor and outdoor contaminants contributing to Sick Building Syndrome or Building Related Illness may include any of the following (abbreviated list):
- VOCs and formaldehyde from building materials or occupational environments
- Microbial VOCs (MVOCs) from wet and actively growing colonies of mold or bacteria
- mold spores and hyphae fragments
- pesticides, fungicides and other biocides
- fuel or refrigerant leaks
- combustion byproducts
- scented cleaning supplies or “air fresheners”
- dander, insect parts and other biological allergens (e.g., cat, dog, mouse, rat, cockroach, dust mite, pollen, etc.)
Sick Building Syndrome and Building Related Illness
If a building owner or tenant suspects a sick building, an industrial hygienist (IH) is usually called in to perform interviews and conduct a sick building inspection. Different companies provide different levels of thoroughness in their inspections, so if you’re concerned you may be in a sick building be sure you select an industrial hygiene expert that is qualified.
In 1984, the World Health Organization (WHO) issued a report suggesting that up to 30% of new and remodeled buildings may have excessive complaints about indoor air quality. That’s NEW & IMPROVED buildings! This is an enormous number of buildings across the world, and the cost (medical and lost productivity) of Sick Building Syndrome is staggering.
New LEEDv4 IAQ Assessment (LEED IAQ Testing) credit ensures that furnishings are installed prior to testing. Furnishings can really stink – and it used to be optional to have furniture installed during IAQ Testing.
Healthy Building Science is an environmental consulting firm providing indoor Sick Building Inspection Services for Building Related Illness and Sick Building Syndrome for commercial, multi-family buildings, offices, industrial and manufacturing workplaces, hospitals and medical facilities, and single-family homes in the greater San Francisco Bay Area and all of Northern California.
An adage to close with –



